Serious paediatric cervical spine injuries (CSI) following blunt trauma are uncommon and those that are unstable generally result from high force or high angular momentum or distraction.
Within the subgroup of children with severe injury mechanisms, particularly those with altered conscious state, radiological signs of spinal injury may be subtle, and clearance may require clinical, radiological, and spinal expertise.
Risk factors for CSI include high-risk motor vehicle accident (MVA), diving or other axial load, medical conditions predisposing to CSI, substantial torso injury, altered mental status, focal neurological deficit, neck pain and traumatic torticollis.
Seatbelt-restrained infants who experience a sudden, massive deceleration are particularly at risk of CSI due to a proportionately heavy head and poor cervical musculature.
Imaging is only recommended for children with risk factor/s identified on careful assessment.
Soft collars are recommended. Hard collars are of no known benefit and potentially harmful.
Seek senior emergency advice if symptoms persist, regardless of radiological findings.
Suspect acute cervical facet joint dislocation in a patient who presents with history of a low velocity, high force injury with a combination of hyperflexion and loading e.g. rugby scrum collapse, abnormal focal neurology suggestive of cord injury, and normal conscious state.
Seek urgent Orthopaedic advice (onsite or via Retrieval Services Queensland (RSQ) if suspect acute cervical facet joint dislocation or spinal cord injury.
Purpose
This document provides clinical guidance for all staff involved in the care and management of a child presenting to an Emergency Department (ED) in Queensland with a possible cervical spine injury following blunt trauma.
This guideline has been developed by senior ED clinicians and Paediatricians across Queensland, with input from Orthopaedic and Spinal surgeons, Queensland Children’s Hospital, Brisbane. It has been endorsed for statewide use by the Queensland Emergency Care of Children Working Group in partnership with the Queensland Emergency Department Strategic Advisory Panel and the Healthcare Improvement Unit, Clinical Excellence Queensland.
Introduction
Serious paediatric cervical spine injury following blunt trauma is rare, occurring in approximately 1% of all paediatric blunt trauma cases, with incidence ranging from 0.4% in the preschool population to 2.5% in the adolescent age group.1, 2 Of these injuries, the majority are stable injuries, while approximately 35% have varying degrees of instability requiring bracing or operative fixation.3
Severe cervical spine injuries generally occur from high-risk mechanisms and present with clinical red flags. Owing to the complexity of radiological interpretation and assessments of stability, and the large ‘denominator’ of children with blunt trauma, there is a critical need for stepwise risk stratification, so that greater expertise and imaging with higher radiation or more sophisticated modalities is reserved for higher-risk children and mechanisms.
The traditional cervical spine clearance algorithms (NEXUS and Canadian C-Spine Guidelines) have demonstrated significant value in assessing adult populations. However, the Canadian C-Spine guidelines have not been validated in children and the Viccellio analysis of the NEXUS rule in 3065 blunt trauma paediatric patients to age 18, included only 30 children with cervical spine injuries, and only 4 under 9 years of age. The PECARN multicentre case-control analysis of factors distinguishing 540 cervical spine injuries in children aged under 16 years, and subsequent prospective study of over 4091 children4 provides the most paediatric specific evidence available and forms the basis of this guideline. Results from a larger child specific PECARN prospective study are expected in the next year or so, and are expected to inform future guidelines. The Australia/NZ multicentre SONIC study (recruitment commenced in 2021) will in future provide better understanding of the use and value of these three risk factor sets in our local paediatric population. Meanwhile it is important to ensure a broad interpretation of their model and to be aware of other mechanisms known to be associated with spinal injury including falls, tumbling and trampolining.
A review of paediatric CSI cases at the two Queensland children’s hospitals during the six-year period of 2008-2013 identified 38 patients aged less than 16 years who sustained a severe spinal injury requiring neurosurgical input (fractures, dislocations, spinal cord injury or combination of these, with input being surgery, traction, brace or plaster fixation). Of these 38 patients, 18 were 8 years of age or younger, and all patients in this age group had occiput-C2 lesions. In patients aged 9-16 years of age, 8 out of 20 had low velocity “facet joint dislocation” type injury.5
Assessment
Emergency care should always involve a rapid primary survey with evaluation of (and immediate management of concerns with) airway, breathing, circulation and disability (ABCD) followed by a thorough secondary survey. Pay specific attention to the maintenance of neutral spine positioning.
Patients with suspected CSI or high risk traumatic injury transferred from other hospitals should have a full C-spine assessment undertaken on arrival in ED or ICU, in view of the high risk of subtle or occult injury.
History
History is critical in the risk assessment of paediatric patients with suspected CSI. Questioning should include information on:
mechanism of injury
past medical history (see below for conditions that may predispose to CSI)
symptoms post-incident including neurological symptoms, neck pain, ambulation and respiratory distress.
Conditions that may predispose to CSI
Down syndrome (shallower facet joints and hypotonia causing increased risk of horizontal displacement)
Klippel-Feil syndrome
achondroplasia
mucopolysaccharidosis
Ehlers-Danlos syndrome
Marfan syndrome
osteogenesis imperfecta
Larsen syndrome
juvenile rheumatoid arthritis
juvenile ankylosing spondylitis
renal osteodystrophy
rickets
history of CSI or cervical spine surgery
occult congenital deformity such as os odontoideum (a congenitally short odontoid peg limiting the effectiveness of the transverse ligament)
Examination
Alert
Do NOT reposition a conscious child with torticollis unless there are airway concerns. Seek urgent Spinal Fellow advice if an unstable fracture/dislocation severely compromising spinal canal diameter is identified on imaging.
Pain vs tenderness
A traumatic cervical spine injury like any other traumatic deformation causes the conscious infant, child or adolescent to be acutely aware of pain and dysfunction, and to protect the area with muscle spasm. The PECARN study found a complaint of neck pain to be a significant risk factor for CSI while midline “tenderness” was NOT associated with CSI. Asking children (where appropriate) where they are sore, and assessing posture, mobility and clinical responses can help differentiate pain from tenderness.
Active range of motion
An assessment of active range of motion is only recommended for patients with no pain, no abnormal neurology, and no altered conscious state as an indication for imaging. While active neck rotation to 45⁰ bilaterally is considered an appropriate range of motion in adults, asymmetrical or painful limitation of movement at 45-90⁰ may be significant in children.
Assessing infants and young children
Assessment of infants and young children presents a particular challenge for the clinician. While relevant history may be obtained from parents or other witnesses, subjective description of symptomatology is unreliable and difficult. History and objective examination findings must be synthesised to determine the need for investigations and/or observation.
In general, CSI in young children is very rare: a 10-year review of more than 12,000 cases of blunt trauma from 22 Trauma Registries in USA identified only 83 children aged up to 36 months with CSI. All children had at least one of the following features: MVA, GCS less than 14, GCS eye = 1, reduced neck mobility, or face or skull fractures.6
The radiation risk in this age-group is higher while the sensitivity of plain films for injury or instability is lower. Assessment of the young child and interpretation of the young child’s radiology may require a high degree of sophistication and experience.
Risk factors for significant CSI in children
high-risk motor vehicle accident (MVA) includes head-on collision, rollover, ejection from vehicle, death in same crash, or speed in excess of 88km/hour
axial load to the head e.g. diving, trampolining, falling from a height
forced neck hyperflexion (low velocity, high force) e.g. rugby scrum collapse, clotheslining
altered conscious state (GCS<15, AVPU <A, intoxicated, confused)
traumatic torticollis (a preference for a rotated position and/or a decrease in cervical spine range of movement, difficulty moving the neck)
respiratory symptoms (includes distress and decreased saturations)
focal neurological deficit (paraesthesia, loss of sensation, motor weakness, or other e.g. priaprism)
other specific features of spinal cord injury such as unexplained refractory hypotension
neck pain (see pain vs tenderness section above)
Acute cervical facet joint dislocation
Patient (typically adolescent) presents with:
history of a low velocity injury with hyperflexion or axial loading (e.g. rugby scrum collapse)
abnormal focal neurology suggestive of cord injury
normal conscious state.
The abnormality is readily apparent on plain films. Time to traction/reduction is critical.
Seek urgent orthopaedic advice (onsite or via RSQ) if suspect acute cervical facet joint dislocation or spinal cord injury.
Thoracolumbar spinal injury
Risk factors include:
high velocity MVA particularly if sash or harness restraint devices have not been worn
ejection from MVA
high speed motor bike/bicycle collisions in which patient has gone over handlebars landing on head prior to impact
multi-trauma victims with unclear mechanism of injury and altered conscious state
abnormal focal neurology
localised thoracolumbar pain
spinal injury at other levels
Investigations
Imaging is associated with radiation risks (exact exposure dependent on the machine used and site-specific protocols) and interpretation of findings can be complex. Imaging based on risk approach is recommended. Analgesia and reassessment prior to immediate imaging may be an appropriate management strategy in some children.
The risks and benefits of each imaging modality needs to be carefully considered. While in adult populations CT is generally preferred where available, this is not routinely recommended in children due the increased risks associated with radiation and the potential need for sedation.
Imaging to identify CSI in children
Considerations for each imaging type are outlined below.
Plain films
sensitivity estimated at 90% but may be as low as 75% in age 0-3 years with severe mechanisms, as distraction failure in the occiput-C2 region is not readily apparent on plain films
10-20% of radiation exposure when compared with CT scan
three views (antero-posterior, lateral and odontoid peg) where technically feasible, increase the sensitivity to detect clinically-significant CSI compared to fewer views
odontoid peg views are technically difficult (may be obscured by teeth or occiput)
able to identify malalignment e.g. facet joint subluxation/dislocation in sagittal view and torticollis in coronal plain view
Of the 542 children with CSI in PECARN, 18 had no abnormality detected on plain films. However, all had at least one risk factor for CSI. The four who required operative stabilisation presented with abnormal focal neurology following a high-risk mechanism of injury (os odontoideum and fall/flip (n=2), atlanto-occipital dislocation from MVA (n=1) and unilateral facet fracture/dislocation (n=1) following a trampoline fall.7
CT scan
gold standard for identifying bony injury
sensitivity to detect significant CSI in children is not 100% as findings can be subtle (e.g. small avulsion demonstrated in a single slice of a CT series). Careful assessment of overall risk is important
potential cancer risks exist from the ionising radiation:
CT scans have been estimated to triple the risk of leukaemia and brain cancer – 10 years after the first CT scan in children less than 10 years of age, one excess leukaemia case and one excess brain tumour case per 10, 000 head CT scans is estimated to occur.8
extrapolation of physical data for radiation exposure during imaging on models at QCH demonstrated that the risks are greater in younger children and females, and that the radiation in a cervical spine CT series has an effective thyroid radiation dose approximately 10 times that of the 3-plain film series.9
MRI scan
superior sensitivity for identifying ligamentous and soft tissue injury, particularly infants with high energy mechanisms10
MR angiography
can identify vertebral artery injuries that may be associated with CSI
consider in the following children:
high cervical spine injuries
fractures involving transverse foramen
neurological signs suggestive of vertebral artery insufficiency including vertigo, mental state changes or unilateral weakness
Decision making should include radiological and spinal teams in consideration of the risks of imaging and of potential treatment in the clinical context. In practice anticoagulation would rarely occur due to the severity of associated blunt trauma.
In view of the above considerations and the availability of local resources, general recommendations are outlined below.
Imaging to identify CSI in children
Imaging type
Utility
Plain films
consider AP, lateral and if possible, open mouth peg view as a screening tool in the conscious population with low pre-test probability of CSI. As normal X-rays further lower the probability of significant spinal injury, these children may then be allowed to actively mobilise with a second stage clinical clearance identifying those with persistent abnormal range of movement or pain.
open mouth peg views are recommended in children aged 5 years or older.
reassess child with careful attention to history and evolving clinical findings before repeating inadequate scanning to avoid unnecessary radiation exposure.
CT scan
consider as first-line investigation in patients with highly concerning mechanisms or clinical features such as persistent focal neurological signs, altered level of consciousness, significant limitation of movement or other serious injuries.
consider CT spinal imaging (either focussed or comprehensive) for better definition in child with persistent symptoms irrespective of plain film findings.
consider a targeted ‘fine cut’ cervical CT scan with reconstructed views if single level concerns.
MRI scan
preferable to CT in the following cases:
child with possible spinal cord or ligamentous injury or SCIWORA (spinal cord injury without radiological abnormality) to provide further information about ligamentous structures.
young ventilated patients requiring prolonged (greater than 48 hours) immobilisation in PICU to augment understanding of CSI risk.
Seek senior emergency advice on choice of imaging for a child with risk factor/s for CSI.
Management
Refer to flowchart [PDF 738.83 KB] for a summary of the emergency management of a child following a CSI.
Spinal immobilisation in children
Immobilisation and spinal precautions are recommended for all children with risk factor/s for CSI until assessment has taken place and CSI has been excluded. Patients at risk of thoracolumbar spinal injury should be kept flat, with neutral positioning of the entire spine and log-rolling.
Infants may be brought into ED having been immobilised in a whole-body vacuum splint. These splints facilitate safe transport from the pre-hospital setting, however must be removed to allow full assessment. This involves deflating the splint, applying a cut-down soft collar if not already applied and log roll for any transfers.
The Queensland Ambulance Service, Princess Alexandra Hospital (PAH) Spinal Injuries Unit and Queensland Children’s Hospital recommend the MOR approach which involves LESS discomfort and risk of pressure complications (the change from stiff to soft collars) but MORE attention to addressing Moments of Risk (MOR) in the smaller number of higher-risk patients.
MOR approach to immobilisation
Specific aspects of the MOR approach include:
soft neck collars
thoracic elevation devices (TEDs) in children aged less than 8 years
lateral sandbags in unconscious patients
careful attention to neutral handling and positioning at moments of risk
Specific consideration in children
Strategies to promote neutral positioning
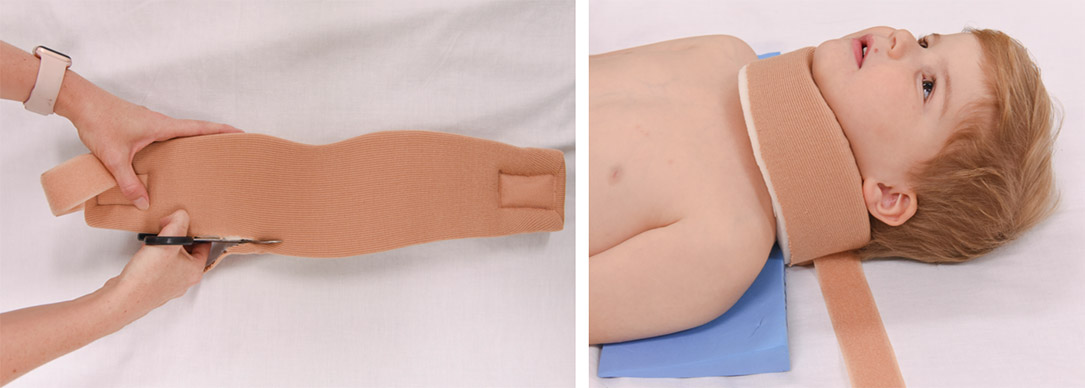
Short submental distance.
Collar needs to be snugly fitted to reduce risk of hyperflexion due to chin slipping (see image below).
Poor tolerance for immobilisation which can lead to agitation.
See table below.
Natural desire to look around.
Position parents at head of bed to avoid hyperflexion.
Cobb angle (the difference in inclination of lines drawn parallel to inferior endplates of C2 and C6) is in the flexed range in a younger child when lying flat.
Position a TED high under the neck when immobilising children less than 8 years of age (see image below).
Neck collars
As with all mechanical trauma to the skeleton, deformations causing spinal cord injury or ischemia occur at the time of the initial massive angulating / displacing forces and are unlikely to be reproduced during normal handling. No orthopaedic immobilisation device can prevent angulation during transfers when high level instability is present, and the differences in angulation between one-piece, two-piece and soft devices with cervical spine precautions during handling is small.11 Standard cervical collars cannot prevent anteropulsion of horizontally unstable injuries, or the risks associated with atlanto-occipital instability.
Soft collars should be used to immobilise the cervical spine. If needed, soft collars can be cut along the lower edge to ensure a snug fit under the chin.
Alert
Hard collars are not recommended. There is no evidence of efficacy.10 Potential harm associated with use include raised intracranial pressure, respiratory disturbance, patient agitation, and soft tissue ulceration.12
Thoracic elevation device (TED)
TEDs are foam wedges designed to improve spinal and airway positioning in children.13
TEDs should be used when immobilising a child aged less than 8 years.
Moments of risk
Moment of risk
Strategies to protect cervical spine
Trolley transfers and log roll
use PAT slide and have nurse/doctor dedicated to head/spine
if less than 8 years of age, use TED on arrival
Pain/agitation
early pain relief
positioning caregiver at head of bed to allow direct eye contact and touch
attendant to reassure and advise family re process
in conscious infants consider removing collar and allowing child to find their own best neck position (e.g. in parent’s arms)
Vomiting
early prophylactic ondansetron
orogastric (or nasogastric if appropriate) insertion
attendant or parent present and “nurse call” for log roll if vomiting
Voiding
log roll girls onto pan to void
boys void into bottle while lying flat
consider urinary catheterisation if unable to clear cervical spine
Imaging
Attendant to:
accompany to X-Ray if removal of collar or manual re-positioning is required
ensure TED used appropriately
ensure CT head and neck position maintains neutrality
Intubation
specific attendant assigned to neck positioning
consider fibreoptic intubation
avoid unpredictable muscular contractions e.g. depolarising neuromuscular blockade agents
Child with no risk factors or pain as only risk factor for CSI
C-spine imaging is not required initially
explain to patient and guardian that the risk of a clinically significant C-spine injury is very low
if required administer Ibuprofen 10mg/kg + Paracetamol 15mg/kg if no contraindications
prop patient up
consider soft collar
observe for 30-60 minutes if neck pain and/or limited range of motion
consider further imaging if neck pain and/or limited range of motion persists on re-assessment
Clinical clearance of CSI
While evidence is limited, CSI can be clinically excluded in a child with no risk factors (including pain) identified on careful assessment (history and examination).
Consider seeking senior emergency advice as per local practice for child with persistent pain.
Child with at least one risk factor/s for CSI other than pain
Seek urgent orthopaedic advice (onsite or via Retrieval Services Queensland (RSQ)) if suspect acute cervical facet joint dislocation or spinal cord injury.
Unstable child
Seek immediate onsite assistance (anaesthetics/critical care/ENT) as per local practice to manage airway.
Seek urgent paediatric critical care advice (onsite or via RSQ) for unstable child.
Manage ABCD as per APLS.
Immobilise with soft collar. If aged less than eight years use a thoracic elevation device (refer to Immobilisation and spinal precautions section below).
Alert
Consider the possibility of neurogenic shock in any hypotensive trauma patient if hypotension persists despite fluid resuscitation and without accompanying tachycardia.
Trauma patients with altered conscious state must be considered at high risk of unstable cervical spine injury +/- spinal cord injury. Recommended actions include:
where possible, document all four limb movements/sensorimotor responses prior to paralysis for ventilation
exercise care when interpreting cervical spine imaging as even CT evaluation may fail to identify ligamentous instability
monitor mean blood pressure with a rigorous and interdisciplinary evaluation of hypotension
consider neurogenic shock (characterised by persistent and refractory hypotension without accompanying tachycardia) while simultaneously actively pursuing other traumatic causes of haemorrhagic shock
consider cerebral and spinal perfusion pressure to avoid secondary hypoperfusion injury. Inotropic support may be required (on paediatric critical care advice).
Stable child
C-spine imaging is recommended (refer to Investigations)
administer Ibuprofen 10mg/kg + Paracetamol 15mg/kg if no contraindications as required
reassess child (including active range of motion) if no abnormality is detected on imaging
Prompt referral to local orthopaedic team is required for child with abnormality detected on imaging.
Seek senior emergency/orthopaedic advice as per local practice for a child with no abnormality detected but ANY of the following:
altered mental status
focal neurological deficit
persistent neck pain
persistent torticollis
CSI clearance
CSI can be excluded in a child presenting with risk factor/s with:
no abnormality detected on imaging
AND
no persistent symptoms during observation period including:
altered mental status
focal neurological deficit
neck pain
torticollis
Following CSI clearance:
explain to patient and guardian that the risk of a clinically significant C-spine injury is very low
remove splinting and cease spinal precautions
recommend sitting posture and encourage gradual mobilisation
In practice many of these children are slow to mobilise particularly if they have been transported with spinal injury precautions.
Escalation and advice outside of ED
Clinicians can contact the services outlined below to escalate the care of a paediatric patient as per local practices.
Child who is unstable or requiring time-critical care
Maintain a high index of suspicion for acute cervical spine instability in a seat-belt restrained infant involved in a high force rapid deceleration injury, even if initial imaging appears normal.
Suspect acute cervical facet joint dislocation in the older, conscious child who presents with the following:
history of a hyperflexion and loading injury e.g. rugby scrum collapse
abnormal focal neurology suggestive of cord injury
Alert
Time-critical care is required in child with:
acute cervical facet joint dislocation- aim for reduction within four hours
Consider discharge for patients in whom CSI has been excluded providing there are no other concerns.
On discharge parents/caregivers should receive appropriate advice regarding analgesia and expected recovery (which may take weeks).
Follow-up
with GP within a week.
Patients who have been assessed by the orthopaedic or spinal team may be discharged home for early outpatient review, with or without ongoing immobilisation, at the subspecialty team’s discretion.
When to consider admission
Patients with confirmed CSI, altered conscious state or focal neurological deficits require admission with spinal immobilisation and spinal precautions until function can be adequately assessed. Clearance of these children is a multidisciplinary responsibility requiring input from PICU, radiology, and spinal services. Handling to maintain neutral positioning and minimise pressure effects can be challenging.
Children in whom there are persistent symptoms such as pain or torticollis despite normal initial imaging may require a period of admission at the discretion of the treating specialist team.